Currently my doc didn’t comment on my Prolactin but i don’t really care, it’s probably due to mk-677.
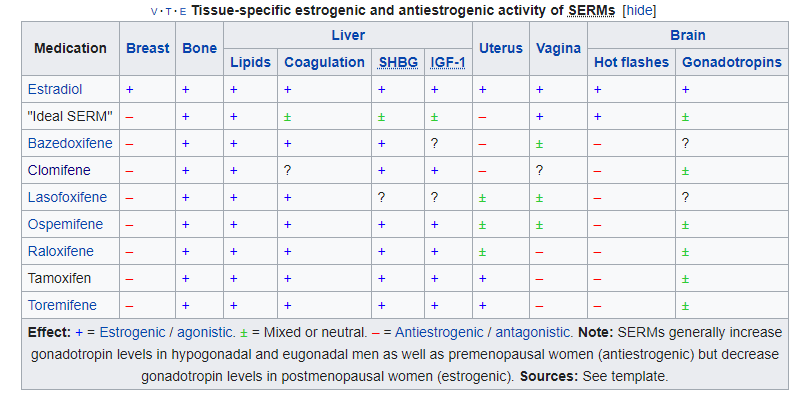
I did. I checked out many studies and also i saw that chart too. However there isn’t much data on Enclomiphene. What makes me hold at this moment is this:
However, one in vitro study in 2007 and later an in vivo study in 2008 have shown that tamoxifen induces apoptosis in growth plate chondrocytes, reduces serum insulin-like growth factor 1 (IGF-1) levels and causes persistent retardation of longitudinal and cortical radial bone growth in young male rats, leading the researchers to express concern giving tamoxifen to growing individuals.[107][108]
But same page also states this:
When tamoxifen was launched as a drug, it was thought that tamoxifen would act as an ER antagonist in all tissue, including bone, and therefore it was feared that it would contribute to osteoporosis. It was therefore very surprising that the opposite effect was observed clinically.
Another source from another site: Studies in vitro and in animals have shown that the effects of tamoxifen on bone resemble those of estrogen. It reduces bone resorption and turnover, stimulates bone formation, and prevents bone loss after oophorectomy.8 9 10 11 12 13 14 15 Its effects in humans are less clear; data from longitudinal and cross-sectional studies of small groups of both premenopausal and postmenopausal women have shown no evidence of accelerated bone loss and some evidence of preservation of or increases in bone density.16 17 18 19 20 21 We report the results of a prospective trial specifically designed to address these uncertainties.
NEJM Journal Watch: Summaries of and commentary on original medical and scientific articles from key medical journals Also this study again says: However, the tamoxifen group had a significantly lower median serum alkaline phosphatase level (suggesting decreased bone turnover or bone remodeling) and a significantly lower rate of new bone formation. (What the hell?)
I want new bone formation, that’s why im trying to recover, i want to grow prominent brow ridge, cheekbones and jawline if possible. My brow ridge is very flat. Im not sure if these thing related to those terms about bone health.
I mean, what the hell? This is very contradictory. It is proven Tamoxifen doesn’t affect bone density or bone mineral content, it even increases it in some. But other horrible things i shared about bones are still there.
Considering my biggest concerns, im afraid about this ‘‘persistent bone growth retardation’’ Also i don’t really know stimulating bone formation or reducing bone turnover and resorption is good or bad for me.
PS:
Bone turnover replaces old bone with fresh new bone. When in balance and not excessive, bone turnover is a beneficial feature of skeletal homestasis. However, in the adult, bone turnover is usually not balanced, with bone resorption exceeding bone formation, and sometimos excessive. In these settings, bone turnover can be deleterious for bone (130).
Things are getting just more complex when i dive in. Lastly, are these effects temporary or permanent changes on bones? No one talks about this, im ok if they are all temporary.

{kind=link}