I’m keeping this thread to document what I’m going thru as well as the successes to come. Having spoken to many of you, I think this simple regimen is probably the best way to go.
Before: recently started Scrotal Cream. Good for my drive and slightly more random erections but needed to increase dose significantly and I became uncomfortable with that. In the past, T Cypoinate helped my drive, had stronger erections and I noticed a return of sensitivity…which makes all the difference in the world.
Now: waiting for Cypoinate to arrive… new regimen:
Testosterone Cypoinate 150mg / week (divided into daily injections using an insulin needle, as I can’t stand regular needles!)
Topical Dutasteride to combat hair loss, as I understand probably less sexual side effects to Propecia. Minoxidil once per day. Twice a day minoxidil made my scalp red and sensitive. I’m sure it’s still helping though.
B 100 Vitamin Complex, once per day.
P5P 50mg once a day. I tried twice a day and gave me the shits. Maybe there’s lactose in it? Thought I’d try reducing prolactin a few more points and see if any benefit. Even though my prolactin tested in the norm.
I have a supply of anastrozole but based on everyones feedback, I’m not taking it consistently. Every so often, I’ve had sensitive nipples and have had some gyno, as confirmed by an endo. If I feel the nipple sensitivity, I’ll take a quarter of a 1mg and by day 2 it tends to go away.
Waiting for some labs I just took to come back and will post. A couple of you have suggested trying clomid and have noticed a return of sensitivity….I’m going to keep that in mind.
Took some new labs but these are the only ones ready so far. It’s been a very long time since testing ferritin. Is low normal very common? Also, I took a quarter of a 1mg anastrozole about 3 days prior, which was obviously a mistake…every test I’ve ever taken has had estradiol above the normal range. This test was taken while on Scrotal cream.
The anastrozole can cause hair loss and 73% of women report hair loss while on anastrozole for the treatment of breast cancer.
It’s common for those lacking iron in their diet and for those who are or will become iron deficient.
The thyroid requires a ferritin of at least 70 for optimal thyroid function and the conversion of other thyroid hormones, so the low ferritin is not normal.
Also off TRT my ferritin is 128 without any iron supplementation, however TRT drops my ferritin down to 24 without iron supplementation because someone on TRT uses more iron stores than someone not on replacement therapy.
Yes I would recommend MCH, MCHC, MCV and iron saturation.
When I was iron deficient, the MCHC was at the bottom of the range, MCV was below range, RDW above and iron saturation was 12 with 20 being the absolute bottom of the ranges.
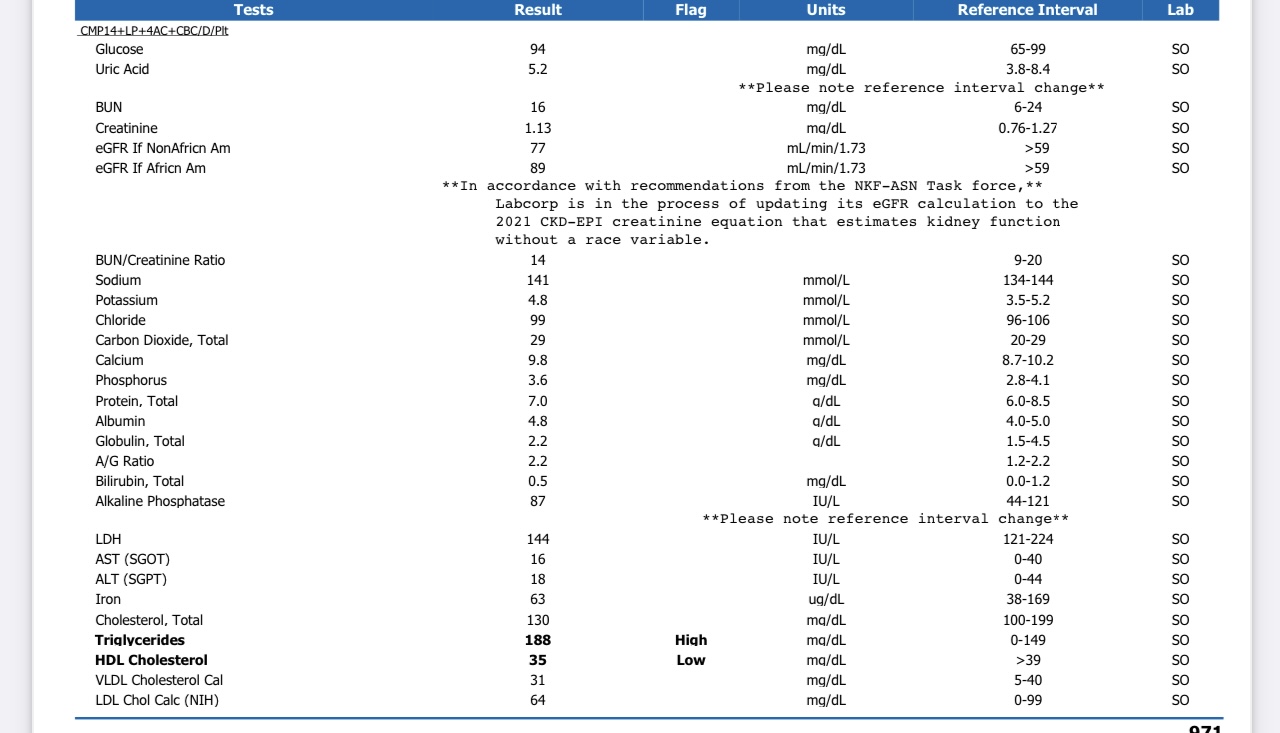
Here’s my latest tests as I’m still doing 4 clicks Scrotal cream in the morning and 4 clicks at bed time until I get the Cypoinate, which they’re telling me is running late for some reason.
New tests from Defy, as I asked about HCG. They basically told me that LH and SBHG may vary as I get settled into T Cypoinate. I recently changed from Scrotal cream to Cypoinate.
She also commented that my Iron was on the lower end but because my hematocrit is higher right now, it wouldn’t be wise to supplement iron, as that can further thicken the blood. Advised me to donate some blood and see if that helps the situation. And if not, lower the T dose a little.
I don’t see how donating blood will help your iron situation, it can make it worse. I supplement 140mg of iron daily and get phlebotomies every 6-8 weeks.
Looks like I worded that wrong. The blood donation is to address the hematocrit level. She said we’ll monitor the iron and as the hematocrit drops to a better level, she may have me start an iron supplement.
Having spoke with Defy recently, here’s my new regimen. Symptoms I explained were:
Low drive
Lack of penis sensitivity (almost none.)
Erectile Dysfunction
Sensitive nipples when on T replacement. Some gyno and was diagnosed as such by an endo.
Blood tests showed lower than normal DHEA.
Blood tests also have traditionally showed higher than normal estrogen and in some tests very high estrogen, especially when the Fractionated Estrogen test was given.
And this is the plan:
Begin Test cyp 200mg/ml .10ml SQ daily
Begin DHEA 15mg Daily
Begin Pregnyl 400IU SQ twice weekly
Begin Anastrozole 0.25mg 1-2x per week for S/S of high E2
Begin Fish oil 3gm Daily (Designs for health, pure encapsulations)
Confused. My hematocrit was 52 about 2.5 weeks ago. The feeling was it was due to the relatively high Scrotal cream dose I was on. I’ve since switched to injections at 150mg / week, taken daily.
I asked Defy if I should check my hematocrit again and they said it would g really change for another 3months, so wait until then. I checked it anyway and it’s down to 48.
Since seeing the high hematocrit just over 2 weeks ago, I’ve been drinking much more water than usual. Could the consumption of all that extra water have lowered the hematocrit in just two weeks?
Also…with this in mind, should I still plan to donate some blood to be on the safe side?