That is probably the only thing I refuse to change with high SHBG!
You may not need to if you can dial in your protocol a free up some free T, veggies have other health benefits.
So it’s been 6 days since my first injection of test cyp 200mg, and goddamn, I wish I had done this years ago. Feel better than I have in a long time. I am sleeping great, even though I cut my dose of trazodone in half. I have taken klonopin only once, and really haven’t felt the need to take it. Dexedrine seems more effective, and I seem able to focus much better even without it.
I am getting hit with some exhaustion though, and am wondering if it’s low e2.
When I saw the doc last week, I still didn’t have my e2 numbers due to labcorp and/or my GP’s incompetence. So he didn’t factor it in to the protocol I’m on, which is:
Anastrozole 1 mg oral tablet 1 tablet oral route every other day
Testosterone Cypionate (grapeseed oil) Compounded 200 milligram once a week
Human Chorionic Gonadotropin 1,000 IU every other day , injectable
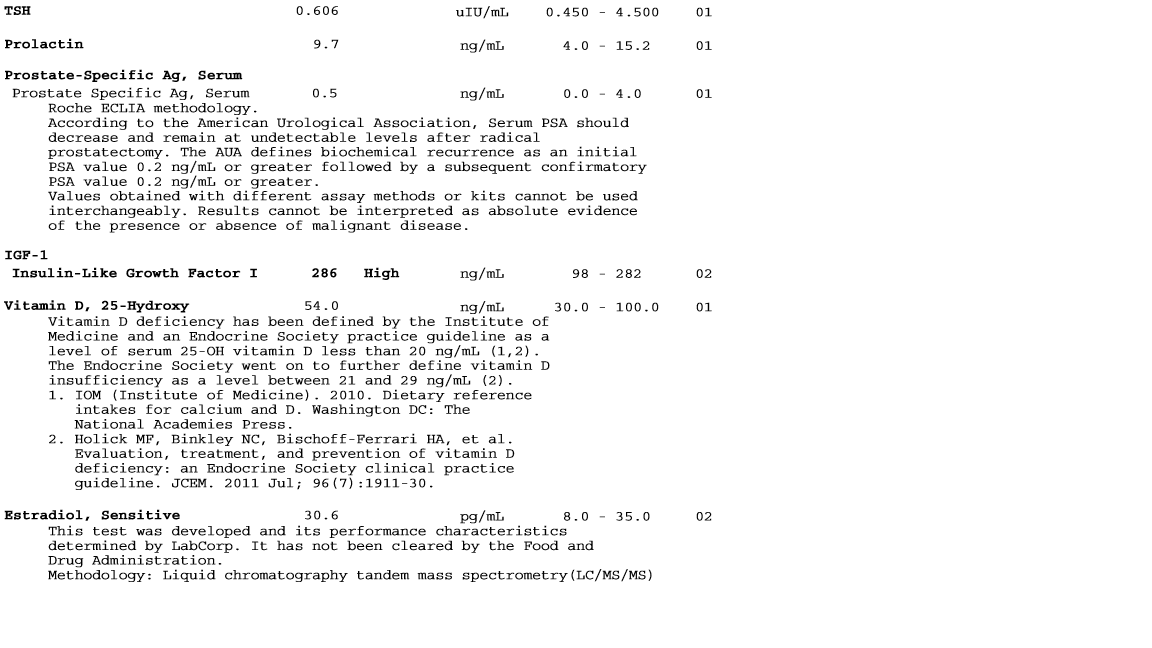
So here’s the thing: I got my e2 labs (finally), and they came back:

I am wondering if perhaps with this new information if the AI dose is perhaps high, or unneeded? Waiting to hear back from doc on this as well, but want to see what you guys think
Stop ai asap. 1 mg EOD is insane. Stop it for a week and maybe resume with taking much less.
1 Like
1mg Arimidex every other day, insane! The rule is 1mg for every 100mg of testosterone per week. Don’t wait for your clueless doctor to respond, this is a clue you need a new one.
I’ll post what the doc says, and then decide if it’s time to move on.
A couple things I am noticing:
-My joints are aching
-I just want to sleep
-I am a bit dizzy and cloudy headed
-not feeling strong like i did the couple days after the first shot
Is this what crashed e2 feels like?
That’s probably what it feels like to have your HPTA shutting down which happens to a lot of us, you have seized control of your HPTA and in about 6 weeks you should start feeling better. I felt like you describe after only 3 days of starting TRT, first 3 days was great!
Got it. I had a shit eating grin on my face all day after that shot. I look forward to getting back to feeling that way!
What accounts for this feeling? What other systems are going offline besides testicular function? I’m guessing there are parts of shutdown that hCG doesn’t help?
I’ve taken a total of 2.5mg of anastrozole, hopefully this won’t be enough to crash my e2 significantly
You need to self inject T twice a week and take anastrozole at time of injections.
TT was strong, and FT was not. That suggests elevated SHBG creating more non-bioavailable SHBG+T that inflates TT so TT overstates your T status while decreasing FT.
Need time of day for cortisol. Should be near 8AM or 1 hour after waking up. AM cortisol=10 is borderline.
You have adrenal fatigue and as that progresses, cortisol could have been high from stress but after time the adrenals can produce lower amounts of cortisol.
You need to post oral body temperatures as suggested below. This is important. Note that two sets of temperature are needed.
In the thyroid basics sticky find references to: rT3, fT3, stress, adrenal fatigue and Wilsons’s Book ← read that.
With a thyroid issue like yours, we can see TRT making things worse as the increased/restored metabolic demands of T can outstrip the metabolic capacity of your body with low thyroid function and lower cortisol levels. There is no simple fix for adrenal fatigue. Taking T4 meds simply increases T4–>rT3. One needs to take T3 only meds to drive down TSH and T4 production. In USA get 25mcg time release T3 from compounding pharmacies.
Get SHBG tested. E2 management is important to influence SHBG levels. Get E2 under control for some weeks before testing SHBG.
Thyroid: We need your history of using iodized salt. Iodine is part of your thyroid hormones.
Magnesium labs: If you get foot or leg cramps or can tense and get a muscle to lock up, your are deficient. See “ZMA” product in this site’s Biotest store.
Never test serum DHEA, only test DHEA-S
We need:
age
height
waist size
weight
Ferritin=80 is considered adequate to support fT4–>fT4 conversion.
fT3 is the only active thyroid hormone, there is no receptor for T4
fT3 should be mid-range=3.2, so you are a bit low.
fT4 as adequate at mid-range
TSH is elevated because of two influences:
- inadequate iodine
- fT3 blocking fT3 at hypothalamus
Please read the stickies found here: About the T Replacement Category - #2 by KSman
- advice for new guys - need more info about you
- things that damage your hormones
- protocol for injections
- finding a TRT doc
Evaluate your overall thyroid function by checking oral body temperatures as per the thyroid basics sticky. Thyroid hormone fT3 is what gets the job done and it regulates mitochondrial activity, the source of ATP which is the universal currency of cellular energy. This is part of the body’s temperature control loop. This can get messed up if you are iodine deficient. In many countries, you need to be using iodized salt. Other countries add iodine to dairy or bread.
KSman is simply a regular member on this site. Nothing more other than highly active.
I can be a bit abrupt in my replies and recommendations. I have a lot of ground to cover as this forum has become much more active in the last two years. I can’t follow threads that go deep over time. You need to respond to all of my points and requests as soon as possible before you fall off of my radar. The worse problems are guys who ignore issues re thyroid, body temperatures, history of iodized salt. Please do not piss people off saying that lab results are normal, we need lab number and ranges.
The value that you get out of this process and forum depends on your effort and performance. The bulk of your learning is reading/studying the suggested stickies.
1 Like
Thank you KSMan.
I will move the content of my other thread here and then request that mods delete it. I am getting a lot out of this forum, so I’ll try to make my case a valuable contribution.
Cortisol one hour after waking:
![]()
Age: 30
Height: 6’3"
Weight: 220lbs
Waist size: 34"
I have not used iodized salt for the most part. Since I first read through the stickies a month ago I started supplimenting 1000mcg iodine, 200mcg selenium daily.
I have used ZMA consistently in the past, and currently take Magnesium threonate before bed
I have not done oral body temps. I will pick up a thermometer and get on that.
Post from other thread:
“Just started TRT to combat high SHBG, I am wondering if the best approach would be to get my E2 numbers into the sweet spot. Should I just skip the AI all together, keep an eye out for high E symptoms, and get bloods done after 6 weeks to see where I am?”
KSMan:
"In a situation like this we associate low E2 with low FT which reduces rate of fT–>E2.
Cortisol=5 was what time of day?
Hard to call your situation. You could try a low dose, 1/8th mg twice a week and see what labs suggest after that.
Liver problems can sometimes lead to high SHBG, your liver labs do not indicate an issue. Sometimes we see guys who have high SHBG with no evident cause.
TT is only part of the story. High SHBG inflates TT with non-bioavailable SHBG+T so TT then overstates T status. I cannot see where FT was tested by itself which is of great interest."
Just a quick question, curious what the consensus here is…
As I am doing these hCG shots EOD, I am wondering why not just inject test with the hCG for more consistent levels? Do both subcutaneously with a single 29" insulin needle? I have seen it suggested elsewhere as an acceptable method…
That would require you to inject HCG once weekly, that doesn’t work as the half life is shorter than test. High SHBG imo shouldn’t do SQ because it supposed to be a smoother release and you need the opposite. It smoothes out the peaks and that’s exactly what you need, large peaks.
1 Like
Interesting. Well I was actually thinking of splitting my weekly test dose into the same EOD hCG injection. But it high SHBG guys need the peak and trough then I’ll stick with what I’m doing.
Nope, you have high SHBG and it require large weekly injections. You don’t want a steady even levels that frequent injections provide, that’s what a low SHBG man wants.
1 Like
Hello @KSman,
I will be doing my followup with my doc after bloodwork to adjust my protocol. I will fully update my thread after that, but before I see my doc… can you elaborate on why I would benefit from twice weekly injections? I want to be able to explain to my doc why this would be better.
You da man.
-Sean
Whenever you inject once weekly your levels peak within 48 hours and start declining after that and one can feel the reduction is levels even though you’re still in range that is almost always felt by the person, you need to maintain stable levels with as little fluctuations as possible. This will keep hematocrit and hemoglobin under control and you won’t feel like your on a rollercoaster.
It’s really insane when you think about it, the patient is having to explain things to the doctor. Lol
1 Like
That’s definitely what I’ve been feeling. Inject on Thurs, feel great on Sat, feel worn out on Wed.
Just an update: got my bloodwork done pre check in with doc, and got interesting results. So because of what you guys said here, for the first couple months I backed off the anastrozole dosage. started showing some signs of high estrogen, mainly bloating and mental fog. Decided to give doc’s 1mg EOD a try… and I will admit, an extra 20mg of test two days before my injections day to feeling so low… I’ve now switched to 100mg E3.5D and feel much better.
After 3 weeks of sticking to that (I hadn’t devated much from it, was doing AI E3D before) I did bloods. Unfortunately I had to do the draw on day 5 and not 6, so it’s not at bottom of trough, but it gives an idea…
My E2 is actually a tad high, having been consistent with 1mg EOD for 3 weeks. Could this be because of the high dose of HCG?
Also, DHT is concerning. I realize that I am missing some tests here, am going to have the more thorough labs from the stickies done soon



Also, has anyone here heard of men using progesterone?
Your TT and FT are way high… if you reduce you test dose you could likely drop the AI. It will take time for your body to normalize. I fought with what I thought was high E2 symptoms for a while and crashed my E2 because of it. I reduced my dose, dropped the AI and I finally feel dialed in a year after starting TRT.