TSH way too high, should be closer to 1.0
tT3 is way below mid-range
fT3 the active hormone has not been tested
Iodine levels should not be too low…
fT3 well above mid-range, TSH is trying hard, but T4–>T3 conversion seems impaired. Ferritin is not causing this.
Any problems with major stress events in your life? [That can increase rT3 that interferes with fT3, increasing TSH and lowering energy.]
FSH is low, average LH probably same. E2 and prolactin are not causing this.
IGF-1 is not great, decent, do not have age to eval. Do not test GH directly, IGF-1 is your GH status. GH released in pulses with short half-life and low results always expected. Was IGF-1 with or without amino acids? If without, there is not problem at all.
Please read the stickies found here: About the T Replacement Category - #2 by KSman
- advice for new guys - need more info about you
- things that damage your hormones
- protocol for injections
- finding a TRT doc
Evaluate your overall thyroid function by checking oral body temperatures as per the thyroid basics sticky. Thyroid hormone fT3 is what gets the job done and it regulates mitochondrial activity, the source of ATP which is the universal currency of cellular energy. This is part of the body’s temperature control loop. This can get messed up if you are iodine deficient. In many countries, you need to be using iodized salt. Other countries add iodine to dairy or bread.
KSman is simply a regular member on this site. Nothing more other than highly active.
I can be a bit abrupt in my replies and recommendations. I have a lot of ground to cover as this forum has become much more active in the last two years. I can’t follow threads that go deep over time. You need to respond to all of my points and requests as soon as possible before you fall off of my radar. The worse problems are guys who ignore issues re thyroid, body temperatures, history of iodized salt. Please do not piss people off saying that lab results are normal, we need lab number and ranges.
The value that you get out of this process and forum depends on your effort and performance. The bulk of your learning is reading/studying the suggested stickies.
Please use an oral thermometer.
Cortisol seems OK, AM vs random unknown. Should be AM cortisol done at 8AM or 1 hour after waking.
Secondary hypogonadism. Read the things that damage your hormones sticky.
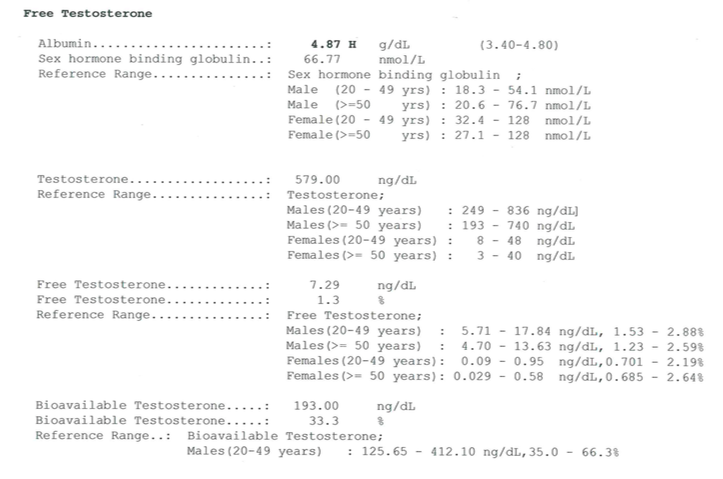
Unexplained high SHBG is creating a lot of non-bioavailable SHBG+T that inflates TT and TT overstates your T status while lowering FT. Docs will be misled by your TT numbers. AST/ALT do not suggest any liver problems that could increase SHBG. E2 increases SHBG but your E2 level is not high to suggest its involvement. More FT of bio-T will reduce SHBG.
Mean cell hemoglobin is high, but nothing else in CBC seems to have any consequence from that.
Lymphocytes seem to be indicating some viral activity which could be immune system business as usual.