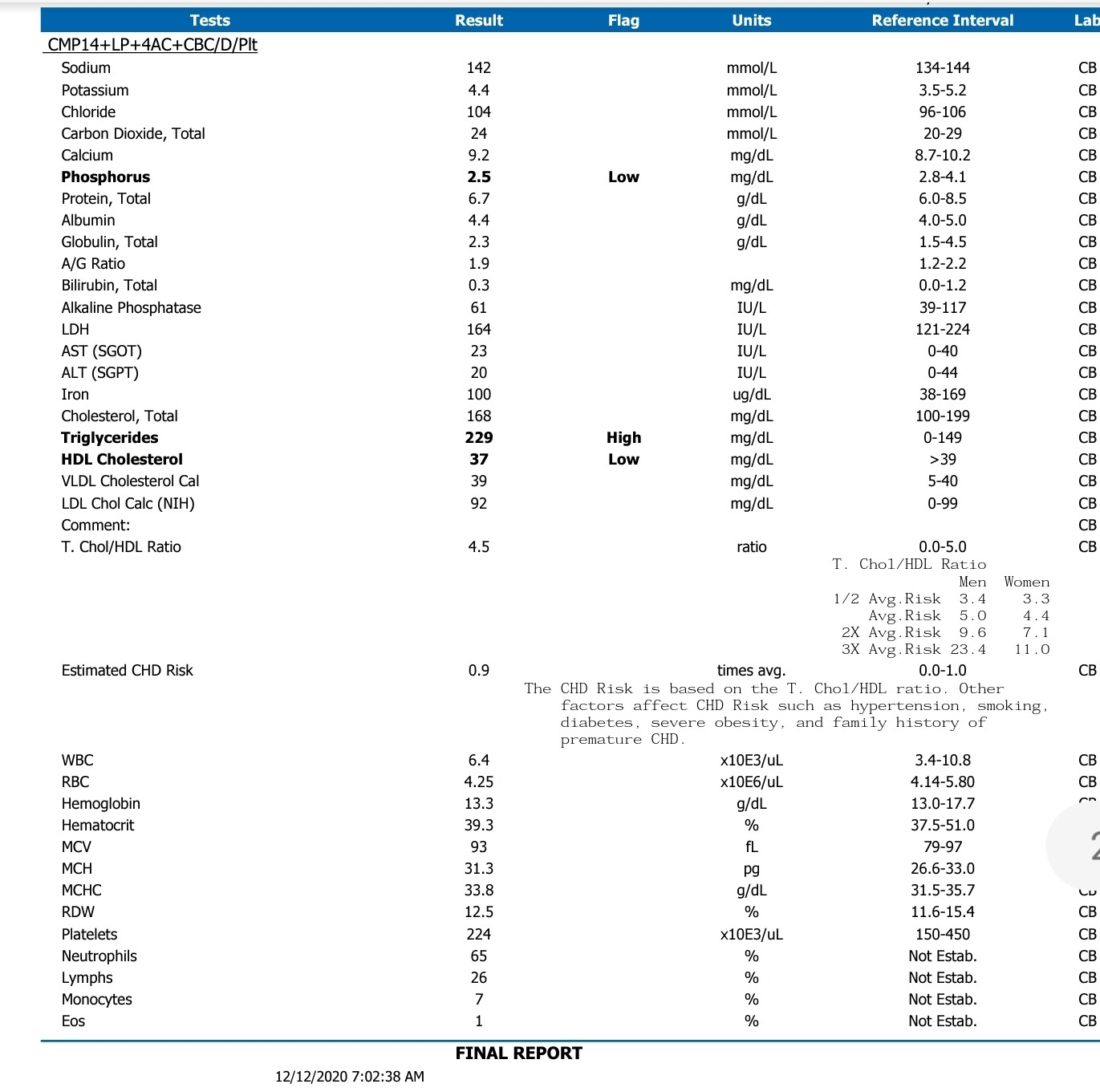
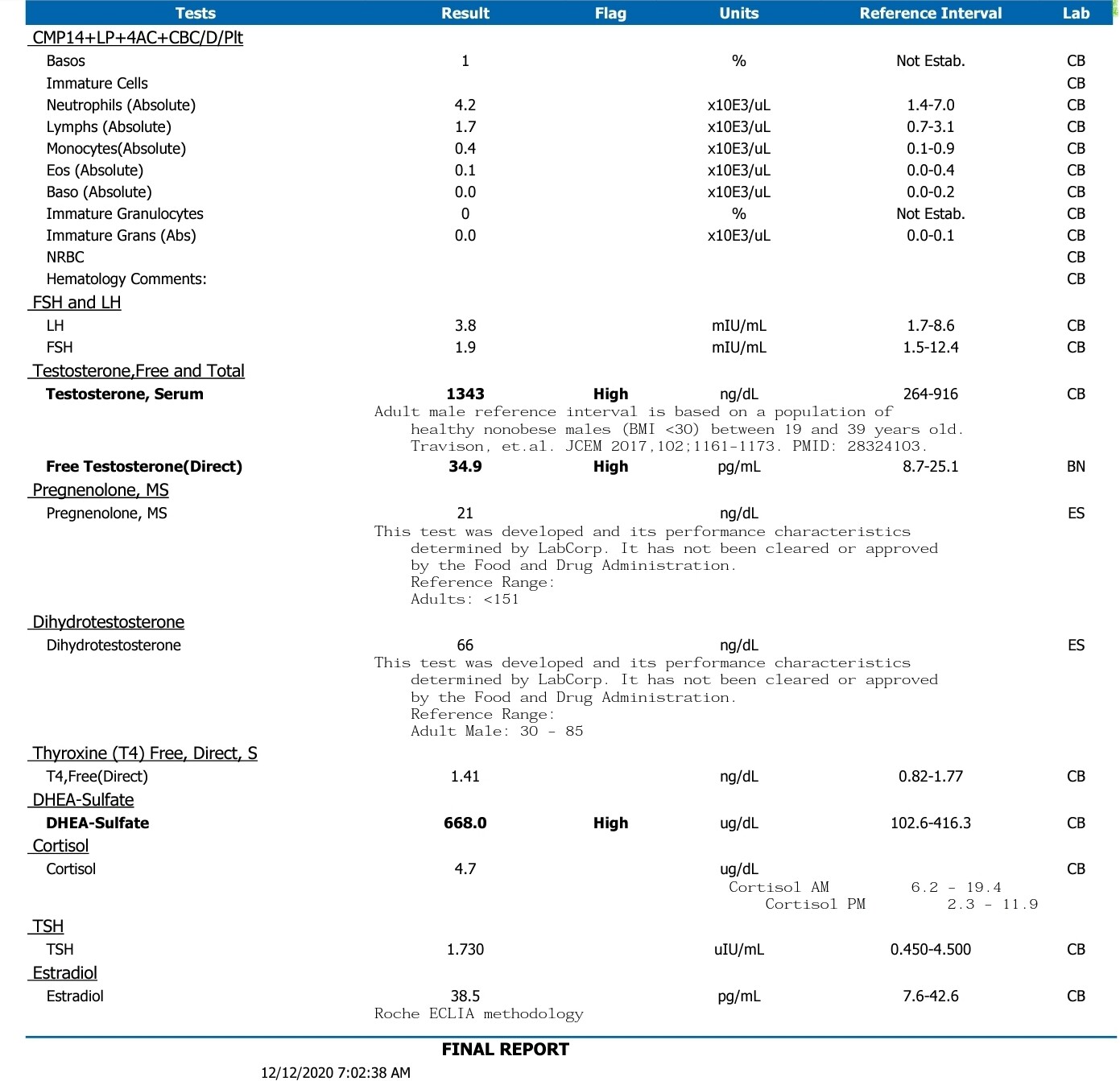
What’s up guys? I’ve been following this forum for quite a while now and wanted to ask your opinion about my protocol, and whether you believe the emerging opinion of an AI never being good to use. I am a testicular cancer survivor and had my left testicle removed several years ago. I then went through several large surgeries due to metastasis, and chemotherapy which did some damage to my right testicle and my thyroid and probably some other things that I’m not so aware of. I started seeing an endocrinologist who placed me on levothyroxine and that made a world of difference for the better! However, for the last couple years I have been experiencing low-T issues. Namely, low libido, low energy, low ejaculate volume, and difficulty concentrating, among others. I know my testosterone level was in the 200s range for a couple different blood draws using the same reference range attached. My estrodial level has consistently been 35 to 38 using the reference range attached. I was told my prolactin has been twice the upper limit normal since chemotherapy, but for some reason they didn’t draw it this time. He is making sure that they will draw it from now on going forward. He wants me to get my labs drawn every 4 weeks. I only have my labs post-TRT, which I have attached here. They will always be drawn between 1:00 and 2:00 p.m… Hear me out here! LOL. I am also on an antidepressant and a opiate-based pain medication. Because of this and other things, I never wake up in the morning and feel good. Even if it’s going to be a good day, I feel like absolute s*** until at least 11am. Even on the days I felt like a god with TRT, it doesn’t start until at least 11:00 a.m. So, with that information, my endocrinologist wanted me to be able to differentiate between feeling good on lab draw days vs bad on lab draw days to help us get dialed into a proper protocol. He confirmed that the most important thing is consistency with time of day when getting labs. Anyhow, 4 weeks before these labs I started with 20mg TC ED SQ, HCG 400iu E4D (for fertility…long shot), and anastrozole (just in case). I really didn’t feel anything different the first week. Then, at the start of the second week I felt like absolute crap. Way worse than I ever did pre-TRT. Me being an idiot and not wanting to wait until my first set of the labs, I took 1/10 of 1mg anastrozole and felt way better. The next day I took the same amount and felt even better. I took the same dose on day 3 and all I can say is I was walking around like King Kong feeling like I was walking orgasm!!! I continued this regimen until the 4-
 week mark when these labs were drawn. I still felt like King Kong when these labs were done so I know this is my sweet spot!! But then I came to the forum and read @dbossa and watched the videos of physicians arguing against the use of AIs, and I didn’t want to take something that was going to ruin my body long term. So, I stopped the anastrozole and continued on. Within a week I started to feel poorly again. It has been one week since and although I feel stronger in the gym I’m not really getting any of the other positive side effects right now.
week mark when these labs were drawn. I still felt like King Kong when these labs were done so I know this is my sweet spot!! But then I came to the forum and read @dbossa and watched the videos of physicians arguing against the use of AIs, and I didn’t want to take something that was going to ruin my body long term. So, I stopped the anastrozole and continued on. Within a week I started to feel poorly again. It has been one week since and although I feel stronger in the gym I’m not really getting any of the other positive side effects right now.

I would love to hear your opinions about AIs. I hear what they are saying but it seemed like it worked wonders in my situation. If it’s absolutely not a good idea to use anastrozole, can you shed any light on protocol changes I can make to feel better given my labs? I really appreciate having this community and look forward to all you guys’ input.
Michael

