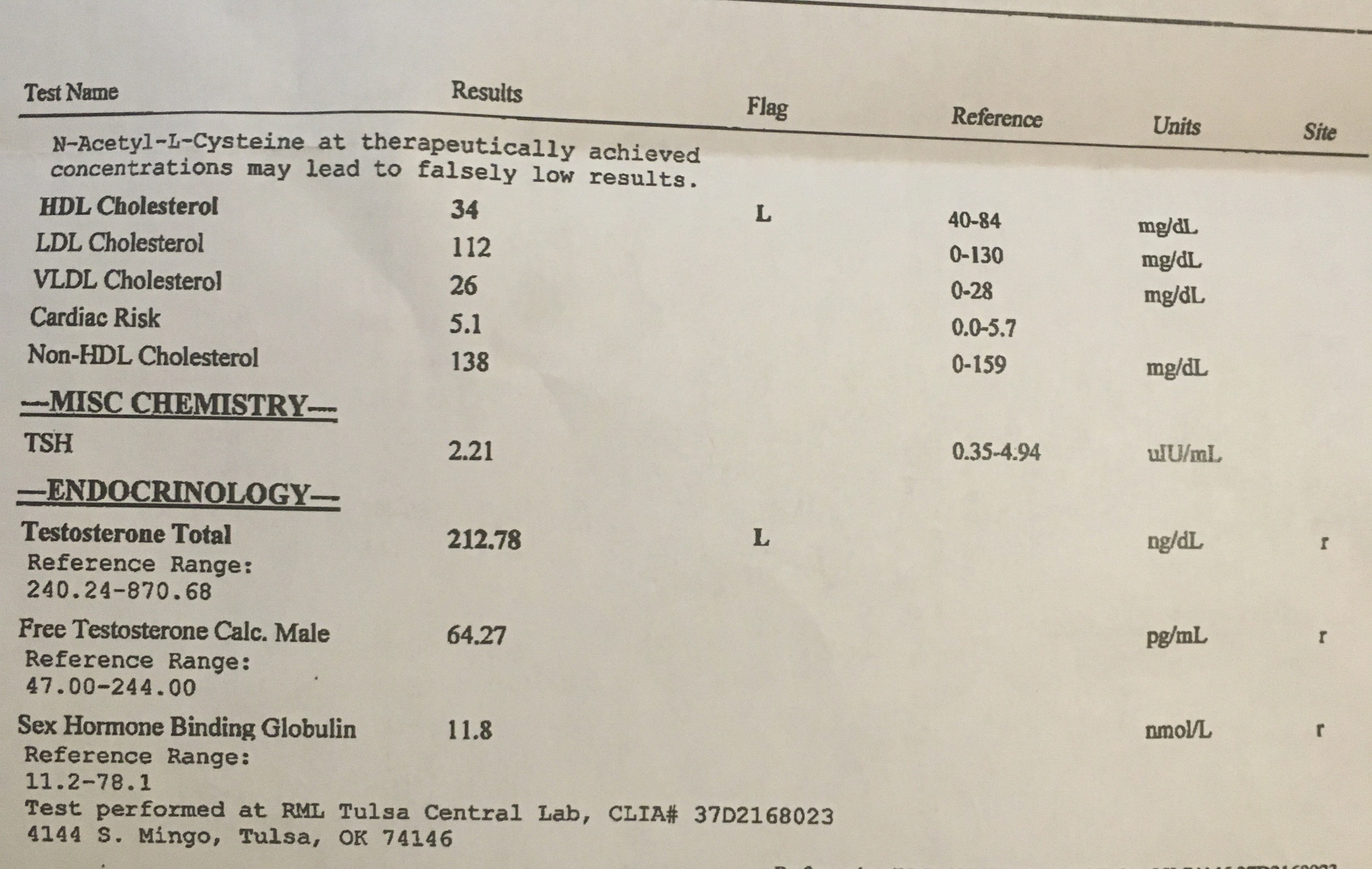
Please help me interpret my initial labs.

38 year old male.
5’10 225lb. ~27-30% bodyfat.
Never been over 200lb until 2020. Weight stayed between 180-190 for years.
Fat is mostly in stomach and love handles.
-Loss of hair on lower legs, skin below the knees is smooth and shiny.
Additional symptoms
Borderline gyno symptoms the last few months. Part of it is the weight but had clear sensitivity / pain in pecs behind nipples.
Long time body temperature regulation issues. Borderline hot flashes. I have been on prescription opiates for years and always assumed the thermoregulation issues were a side effect of RX opiates but I understand hormones can play a factor. I’m frequently hot when others are cold. Occasional hot flashes where I’ll actually break into light sweat but temperature doesn’t increase.
libido comes and goes. It is definitely lower than it should be.
Decent bone structure. Never broken a bone outside of knuckles and toes from martial arts in my youth. Have been getting cavities easier the last 5-10 years.
No issues growing facial hair.
Male pattern baldness runs in the maternal side of my family. I shave my head but there’s a solid quarter + sized bald spot on my crown.
History of prescription stimulant use due to ADD diagnosis.
History of depression on and off since late 20’s. It’s not debilitating depression by any means but the biggest symptom is always social withdrawal.
Current complaints at the top of my list (outside of weight gain) are lethargy / fatigue and really poor physical recovery… if I do a weekend of heavy physical labor I’m eating nsaids like m&ms and walking like an 80 year old. I’m sure the extra weight isn’t helping but this last year sore muscles take twice as long to recover and hurt twice as bad.
Overall my energy is extremely inconsistent. I feel like I have 3 good days a week where I can really kick ass. Other days I struggle to get up the drive and motivation to get up and do work. I’ll lazily work from bed instead of home office on these days and maybe clear 50% of my workload if I’m lucky.
Sleep is pretty bad. I get 7 hours on average but I frequently wake up throughout the night. Half of the time even if I do seem to sleep ok I don’t wake up refreshed.
If I missed anything let me know. I appreciate any insight.
I’m going back in to see the doc that rx’d these labs for me tomorrow. She’s open to TRT via one of the clinics, she doesn’t RX it herself. She’s also willing to request more labs.
Do I need FSH/LH, more thorough thyroid testing? Estrogen / prolactin? Or is what I’ve got here enough to go ahead and reach out about starting a TRT protocol?

